12 Rebuttals To Transgender Ideology - Evidence from Child Development
- @prof_curiosity1
- May 31
- 23 min read
A series of X articles from EBSWA member @Prof_Curiosity1

1) Gillick Competence and the "Transchild"
Gillick competence originates from the 1985 House of Lords decision in Gillick v West Norfolk and Wisbech Area Health Authority. The ruling established that a child may consent to medical treatment if they possess “sufficient understanding and intelligence to understand fully what is proposed.” Its purpose was to balance parental authority with a child’s emerging autonomy in limited circumstances, particularly where withholding care could result in immediate harm. Importantly, Gillick competence was developed for specific, time limited, and low risk medical decisions, where benefits were clear, alternatives few, and consequences largely reversible. It was not intended as a general principle of child self determination, nor as a mechanism for authorising interventions with profound, long term developmental implications.
The contemporary application of Gillick competence to gender affirming care represents a significant departure from this original purpose. Interventions such as puberty blockers and cross sex hormones are not discrete treatments, but interventions that alter the very biological and psychosocial processes through which identity, cognition, and future capacity for consent normally develop.
Child development theory helps explain why this expansion is problematic. Across major frameworks - Piaget, Kohlberg, Erikson, Marcia, and others - the capacities required for informed consent emerge gradually and unevenly. Abstract reasoning, future oriented thinking, appreciation of opportunity costs, and integration of identity over time develop primarily in mid to late adolescence.
Pre-pubertal and early adolescent children typically reason concretely, focus on short term relief, and rely heavily on externally supplied interpretations of distress. Kohlberg’s work on gender development shows that children’s understanding of sex and gender is constructed gradually and tied to cognitive milestones, not the early possession of an internal, self-authored identity. Erikson and Marcia locate identity formation itself within adolescence and emphasise the necessity of exploration prior to commitment. Premature foreclosure, commitment without moratorium, is associated with later reassessment and distress.
From this perspective, asking a child to consent to interventions that fix an identity before the relevant developmental processes have unfolded places the child in an impossible position. Gillick competence assumes that a child can understand the implications of a decision without that decision undermining the developmental processes that would normally deepen such understanding. Gender affirming interventions challenge this assumption directly. By suppressing or redirecting puberty, they intervene in the very developmental pathway through which cognitive maturity, embodiment, sexual orientation, and identity integration typically emerge. This creates a circular ethical problem: the child is deemed competent to consent based on a capacity that the intervention itself may constrain or permanently alter.
In such cases, legal competence risks becoming a procedural shortcut rather than a meaningful safeguard. From a developmental and ethical standpoint, the application of Gillick competence to gender affirming care therefore exceeds its original scope. It shifts the doctrine from a protective accommodation of emerging autonomy to a justification for irreversible or partially irreversible interventions under conditions of uncertainty. A developmentally aligned approach would recognise that uncertainty in paediatrics demands caution, not acceleration. Where identity is still forming, distress is often transient, and long term outcomes remain contested, safeguarding requires prioritising psychological support, exploration, and time. In this context, restraint is not a denial of care, but an affirmation of the child’s right to mature before life altering decisions are made.

2) "Social Transition is harmless"
Social transitioning, changing a child’s name, pronouns, and social role to reflect a cross sex identity, is often presented as a neutral or reversible act. Developmental evidence suggests otherwise. In childhood and early adolescence, social transition functions as a powerful identity intervention that can alter developmental trajectories for the child involved and reshape the social environment for their peers. For the child, social transition risks identity foreclosure. Developmental psychology (Erikson, Marcia) shows that identity formation requires time, exploration, and cognitive maturation.
When a child’s distress is interpreted as evidence of a fixed identity and publicly affirmed as such, exploration narrows. Social transition stabilises/solidifies what would be a provisional self-concept at precisely the stage when flexibility is developmentally normative. Multiple follow up studies and detransitioner accounts indicate that early social transition is associated with higher persistence of gender dysphoria, suggesting not discovery of an innate identity, but rather, consolidation through reinforcement. Cognitive and learning theories help explain why this occurs. Children reason concretely (Piaget), rely on external cues for self understanding, and are highly sensitive to adult authority and peer feedback (Vygotsky, Bandura).
Once a new identity is socially ratified, by teachers, peers, and institutions, it becomes costly for the child to question or revise. Reversal risks social loss, shame, or perceived betrayal, making natural resolution less likely even when distress would otherwise remit.
The impact does not stop with the socially transitioned child. Schools are primary sites of social learning. Introducing the concept that identity is internally self declared and can override biological reality teaches all children a contested model of selfhood at a highly impressionable age. This can blur children’s understanding of their own bodies, lead ordinary developmental differences to be treated as fixed identities, and intensify peer imitation, especially among adolescents, for whom belonging and social status matter deeply.
Peer environments are also altered structurally. Classmates may be required to participate in affirming practices they do not understand, cannot question, or privately doubt, placing them in moral and cognitive conflict. Research on conformity and authority shows that such conditions suppress honest inquiry and promote compliance over understanding. For vulnerable children, particularly those with anxiety, autism, or identity diffusion, this environment may unintentionally signal that distress is best resolved through identity change rather than psychological support.
Finally, social transition reshapes safeguarding norms. Once a child is publicly transitioned, professionals may feel constrained from exploring alternative explanations for distress or revisiting earlier assumptions. This mirrors the evidence gaps identified in the Cass Review (2024): early affirmation can foreclose assessment rather than support it.
Social transitioning is not a benign accommodation. It is an active developmental intervention with foreseeable risks: for the child, premature identity consolidation leading to puberty blockers, cross sex hormones; for peers, distorted models of selfhood and constrained developmental space. Because children are still figuring out who they are, and we cannot know how they will develop, the safest approach is to keep options open: support distressed children without requiring them, or their peers, to act as though a disputed theory about identity is already settled fact.

Rebuttal 3) “I knew I was trans at age four.”
This statement reflects a retrospective adult interpretation of early childhood experience. While such accounts may be sincerely held beliefs, they do not constitute evidence that young children possess an innate, stable gender identity in early childhood, nor that such an identity can be reliably identified or acted upon at that age.
1. Developmental Capacity at Age Four At approximately four years old, children are in the pre-operational stage of cognitive development (Piaget). At this stage: - Thinking is concrete, appearance based, and egocentric - Abstract concepts such as identity, permanence, or internal psychological states are not yet formed - Self descriptions are fluid and highly responsive to immediate context Developmental research (Kohlberg) shows that children of this age can label themselves as “boy” or “girl,” but this reflects categorisation based on external cues, not an internally authored or abstract identity. Even the later stage of sex role constancy (typically 5–7) refers to biological permanence, not subjective self definition independent of the body.
2. Retrospective Meaning-Making Adult recollections of childhood are shaped by: - Later knowledge and conceptual frameworks - Cultural narratives available at the time of recall - Subsequent life experiences A four year old cannot meaningfully conceptualise “being trans” because the category itself requires adult level abstraction. What is often recalled retrospectively may have been: - Sex atypical interests or preferences - Discomfort with gendered expectations - A sense of difference or distress - Identification with opposite sex roles or play These experiences are common in childhood and historically did not predict adult transgender identity.
3. Individual Experience vs. Population Level Evidence An individual adult outcome does not establish: - That the experience was innate rather than constructed over time - That early interpretation was accurate rather than revised - That similar children should receive early social or medical intervention Developmental science and longitudinal studies demonstrate that most children with gender related distress do not persist into adult transgender identification. Policy and clinical practice must therefore rely on population level evidence, not retrospective narratives.
4. Clinical and Ethical Relevance Adult self-understanding cannot be retroactively applied as a diagnostic or treatment justification for children. In paediatrics: - Decisions must be based on what children can understand at the time - Interventions must account for developmental uncertainty - Outcomes must be evaluated across groups, not inferred from individual trajectories Accepting retrospective adult certainty as proof of childhood innateness risks over-interpreting early childhood behaviour and medicalising normal developmental variation.
Summary: Statements such as “I knew I was trans age four” reflect adult meaning making, not evidence of early childhood diagnostic capacity. As personal narratives these anecdotes do not override established developmental science, nor do they justify early identity consolidation or medical intervention in children. That society chooses to imbue them with exaggerated importance reflects more on the values inherent in that society rather than the veracity of the statement itself.

Rebuttal 4) “Better a live son than a dead daughter”
This phrase is frequently used to justify early social or medical transition for gender distressed children on the assumption that non affirmation substantially increases suicide risk. While emotionally compelling, the claim is not supported by the available evidence and rests on several critical misunderstandings.
1. Suicide risk is complex and not causally attributable to non-affirmation. There is no high quality evidence demonstrating that failure to socially or medically affirm a child causes suicide. Elevated suicidality among (gender) distressed youth is strongly associated with pre existing mental health conditions, including anxiety, depression, autism spectrum conditions, trauma exposure, and family or peer difficulties - factors that are highly prevalent in this population. Systematic reviews (including the Cass Review, 2024) have found that claims linking affirmation or medical transition to suicide prevention rely on methodologically weak studies, often cross-sectional, lacking controls, and unable to establish causation.
2. The framing presents a false binary The statement implies only two options: affirm and live, or do not affirm and die. This is a false dichotomy. Evidence based alternatives exist, including: - Comprehensive psychological assessment - Trauma informed psychotherapy - Treatment of comorbid mental health conditions - Family support and environmental stabilisation - Allowing development to proceed without irreversible intervention These approaches have historically been associated with high rates of distress resolution without medicalisation.
3. Medical intervention does not reliably reduce suicide risk Long term outcome data do not demonstrate that puberty blockers or cross sex hormones reduce suicide risk in children or adolescents. Some of the highest quality long term studies in adults show no reduction- or even elevated - rates of psychiatric morbidity and suicide compared to population controls, even after medical transition. Presenting medical transition as suicide prevention therefore exceeds the evidence and risks overstating benefits while understating harms.
4. The statement exerts coercive pressure on parents and clinicians Framing decisions in terms of a child’s death creates moral duress and undermines informed consent. In paediatrics, ethical decision making requires proportionality, uncertainty tolerance, and safeguarding, not fear based urgency. No other area of child medicine treats suicide risk by affirming a child’s explanation of distress as diagnostically determinative without rigorous evaluation.
5. Protecting life does not require affirming a theory. Supporting a child’s safety and wellbeing does not require endorsing a contested explanatory framework about identity. Children can be protected, supported, and kept safe without asking them, or their parents, to accept an unproven theory with irreversible consequences.
Conclusion: The claim “better a live son than a dead daughter” is rhetorically powerful but scientifically unsound. It has been the go to argument of the transactivist movement seeking to push their ideology onto families and children. It conflates correlation with causation, presents a false choice, and places undue pressure on families under distress. The repeated invocation of suicide as an inevitable outcome of non affirmation functions less as an evidence based risk assessment and more as a rhetorical device that weaponises fear, forecloses clinical judgment, and pressures families and professionals into irreversible decisions unsupported by robust data.
A safeguarding oriented, developmentally informed approach recognises that protecting a child’s life and protecting their developmental future are not opposing goals. Evidence based care prioritises both, without resorting to irreversible interventions justified by fear rather than data.

Rebuttal 5: “Trans children have always existed and are born this way”
This claim is frequently presented as self evident, but it does not withstand historical or developmental scrutiny when applied to pre-pubertal children.
1. Absence in a Century of Developmental Observation Across the 20th century, child development was one of the most intensively studied domains in medicine and psychology. Researchers including Piaget, Kohlberg, Gesell, Montessori, Bowlby, Erikson, Winnicott, and others observed hundreds of thousands of children across cultures, settings, and decades. None described a naturally occurring class of pre-pubertal children who: - Persistently asserted an innate, cross sex identity - Framed distress as being “born in the wrong body” - Required social or medical transition as a normative developmental pathway If such children had been common, or even moderately prevalent, they would have been documented. Discovering a new category of child would have been a landmark finding. It did not occur.
2. Historical and Cross-Cultural Misattribution Claims that trans children “always existed” often rely on: - Gender-nonconforming behaviour - Adult "third gender" social roles - Retrospective reinterpretation of historical figures These phenomena are not equivalent to modern claims about young children possessing an internal, abstract gender identity requiring early intervention. Historical and cross cultural gender roles are socially defined, typically apply to adolescents or adults, and do not involve paediatric medicalisation. Reinterpreting past behaviour through contemporary identity frameworks constitutes retrofitting, not evidence of timeless biology.
3. Developmental Constraints Developmental psychology places clear limits on what children can meaningfully experience and articulate: -Young children reason concretely (Piaget) - Gender understanding emerges gradually and is anchored to the body (Kohlberg) - Identity formation requires adolescent cognitive and psychosocial maturity (Erikson, Marcia) An abstract, innate, cross sex identity independent of the body is developmentally implausible in early childhood. Distress may be real, but the explanation given to the child is supplied by adults and culture.
4. Correlations with Social Introduction The sharp rise in transgender identification among children and adolescents coincides with: - The introduction of gender identity concepts into schools - Clinical affirmation protocols - Social media dissemination - Institutional endorsement This pattern is consistent with social learning, schema formation, and reinforcement mechanisms (Bandura, Vygotsky, Bem).
5. What the Evidence Supports The evidence supports the following conclusions: - Children have always shown sex-atypical interests and behaviours - Children have always experienced distress, trauma, and discomfort with puberty - Children have not historically articulated these experiences as an innate cross sex identity The modern concept of the “trans child” represents a new explanatory model, not the rediscovery of an old biological category.
Conclusion: Claims that “trans children have always existed” rely on systematic conflation: behaviour with identity, adult narratives with childhood development, distress with diagnosis, and cultural interpretation with biological fact. Developmental science does not support the claim that children are born with a fixed, innate gender identity independent of sex. What has changed is not children, but the framework used to interpret them. In paediatric care, new theories require strong evidence, not moral certainty. That standard has not been met.

Rebuttal 6: "Gender incongruence is real and not a "fabricated condition."
Children and adolescents experience genuine distress related to their bodies, social roles, peer relationships, puberty, or expectations tied to sex. That distress deserves careful, compassionate clinical attention. What is currently disputed is how that distress should be conceptualised and treated, not whether it exists.
From a developmental perspective, distress is not the same thing as diagnosis, and diagnosis is not the same thing as etiology. Across child development theory, children’s self understanding is known to be fluid, relational, and strongly shaped by cognitive maturity and social context. Piaget shows that abstract, internally coherent identity concepts emerge gradually; Kohlberg demonstrates that early gender understanding is concrete and externally anchored; Erikson and Marcia locate identity consolidation in adolescence, after a period of exploration; Vygotsky and Bandura emphasise the powerful role of language, authority, and reinforcement in shaping how children interpret their experiences; Fonagy highlights limits in reflective self-understanding that persist well into adolescence.
Historically, children presenting with sex-related distress were understood through these frameworks, often involving anxiety, neurodevelopmental differences, trauma, same sex attraction, or difficulty tolerating pubertal change. Longitudinal evidence showed that for many, distress resolved as development progressed.
What is new is not the distress itself, but the explanatory model: the claim that such distress reliably indicates an innate, fixed gender identity that exists independently of sex and can be identified in childhood. Calling this model into question does not deny children’s suffering. Rather, it reflects a core paediatric principle: when development is ongoing and outcomes are uncertain, clinicians must distinguish between lived distress and the theories used to explain it, especially when those theories justify interventions that may foreclose future developmental pathways. The evidence based approach therefore is to acknowledge distress as real, while resisting premature certainty about its meaning or its medicalisation.

Rebuttal 7: “Talking therapy is conversion therapy”
The claim that exploratory talking therapy for gender-distressed children is “conversion therapy” is a category error. Conversion therapy refers to coercive attempts to change a person’s sexual orientation or suppress identity through shame, threat, or force. Ethical psychotherapy does none of these. By contrast, talking therapy in paediatrics is the standard first line approach precisely because children are still developing.
Across major child-development frameworks, identity is not treated as a fixed essence that must be affirmed on demand, but as something that emerges through maturation, embodiment, and social learning:
Piaget shows children’s reasoning is concrete and present-focused long before adolescence; they cannot reliably evaluate abstract, lifelong trade-offs.
Kohlberg describes gender understanding as a gradually acquired cognitive concept (constancy), not an innate inner identity.
Erikson and Marcia locate identity consolidation in adolescence and warn that premature commitment without exploration produces foreclosure, not healthy identity.
Vygotsky and Bandura show that children absorb identity frameworks through social mediation, modelling, and reinforcement—making them especially vulnerable to adult-led narratives.
Fonagy demonstrates that reflective self-understanding (mentalisation) develops over time, and is often impaired under stress, trauma, or neurodevelopmental difference.
In this developmental context, therapy is not an attempt to “make a child cis.” It is an attempt to: 1. reduce distress 2. assess comorbidities (autism, trauma, anxiety, OCD, eating disorders) 3. strengthen coping and family support 4. preserve developmental flexibility while outcomes remain uncertain. Calling therapy “conversion”, functions rhetorically to shut down clinical inquiry. It treats one interpretation of distress, innate "gender identity", as unquestionable, and recasts exploration as moral wrongdoing.
In childcare, evidence based psychological support is not a threat, it is the ethical baseline.

Rebuttal 8: “Puberty blockers are safe, they’re used for precocious puberty”
This argument sounds persuasive, but it relies on a false equivalence. Puberty blockers (GnRHa) are used in precocious puberty for a fundamentally different purpose: to pause abnormally early puberty and allow normal development to resume on time. In other words, the treatment is used to restore the typical developmental trajectory and reduce risk. In paediatric gender medicine, the goal is different: to interrupt normal puberty in otherwise healthy adolescents in order to change (or prevent) sexed development. That is not the same clinical scenario, ethically or biologically. Key differences:
1) Different patients, different baseline risk Precocious puberty patients are not being treated for identity distress. They are being treated for an early onset endocrine condition. The risk benefit calculus is not transferable.
2) Different duration and developmental timing In precocious puberty, suppression is usually shorter and aimed at delaying puberty into the normal range. In gender medicine, suppression often occurs at the exact developmental window where puberty drives: - bone mineralisation - brain maturation - sexual development - psychosocial and identity consolidation (Erikson/Marcia)
3) Different clinical pathway In gender services, puberty blockers are frequently described as a “pause,” but in practice they often function as the first step in a pathway leading to cross sex hormones. That makes the intervention developmentally and ethically non neutral.
4) Safety claims exceed the evidence The core problem is not that risks are unknown in principle, it’s that long term outcomes are not well established for this indication. This is exactly why the Cass Review and other independent evaluations judged the evidence base as low or very low quality.
5) Developmental psychology matters Child development theory predicts that identity and meaning making are still forming during puberty. Pausing puberty may alter the conditions under which a young person: - integrates their body into self-concept (Piaget) - consolidates identity through exploration (Erikson/Marcia) - matures in future-oriented reasoning and consent capacity So the question is not simply “Is the drug safe in another condition?” It is: Is it safe and beneficial to interrupt normal puberty for this purpose, in this population, at this stage of development? That has not been demonstrated.
Conclusion: “Used in precocious puberty” does not establish safety or ethical justification for routine use in "gender distressed" adolescents. Different condition, different developmental stakes, different evidence standard.
TL;DR - Apples and pears are indeed similar looking fruits; but to say, on the basis of that categorisation, that they are the same, is ludicrous. A false equivalence.

Rebuttal 9: “Regret is Rare”
A common justification for paediatric transition is the reassurance that regret is rare. It is used as proof that gender affirming care works, that early intervention is safe, and that safeguarding concerns are exaggerated. But when assessed through child development theory, evidence quality, and basic paediatric ethics, the “rare regret” claim does not meet the standard required for irreversible or development altering interventions.
1. “Low Regret” Is Not the Same as “Good Evidence” In paediatrics, long term outcomes matter most. Yet much of the research used to claim low regret is characterised by: - short follow up - high attrition and loss to follow up - weak tracking once patients disengage from services - outcome measures that prioritise clinic retention over long term wellbeing A low regret rate cannot be confidently claimed if large numbers of participants disappear from the dataset.
2. Regret Is Often Defined So Narrowly It Becomes Invisible Many studies count regret only when a patient returns to the same clinic and explicitly states it. But regret and harm often appear differently in real life: - silent disengagement - returning to live as one’s sex without re contacting services - grief over infertility or sexual dysfunction - psychological distress reframed as unrelated anxiety or depression - complications managed privately rather than reported If regret is defined narrowly, it will inevitably appear rare.
3. Child Development Does Not Support the Stability Assumed by This Argument The “regret is rare” narrative relies on an assumption that children can possess a stable, self authored cross sex identity early enough to justify medical intervention. But major developmental frameworks do not support this. Piaget: Abstract identity claims require maturation Piaget’s work shows that children’s thinking is initially concrete. Abstract reasoning about permanence, identity, and future consequences develops gradually and typically strengthens later in adolescence.
Children may feel strongly, but that is not the same as understanding what they are committing to. Kohlberg: gender constancy is not “inner gender identity” Kohlberg describes how children gradually understand sex as stable across time. His theory does not describe a developmental stage where children naturally conceptualise sex as separate from the body. Erikson and Marcia: identity consolidation occurs later Erikson locates identity consolidation in adolescence. Marcia emphasises exploration before commitment. A key risk is identity foreclosure, early commitment without exploration, which is associated with poorer outcomes. Many detransitioner accounts resemble this developmental pattern.
4. “Low Regret” Data Often Comes From the Wrong Population Much of the low regret narrative is based on older adult cohorts, often: - male - carefully screened - with long histories of dysphoria - in a very different clinical and cultural environment This is not comparable to the current paediatric referral population, which includes large numbers of adolescent girls with high rates of anxiety, autism traits, trauma, and peer influence effects.
5. Developmental Suggestibility Makes Regret a Lagging Indicator Child development theory also explains why regret may appear low in the short term even when harms are real. Vygotsky and Bandura show how children acquire identity frameworks through social mediation, modelling, and reinforcement. When an identity is rewarded and institutionally affirmed, immediate relief is common. But relief is not proof of truth. It is often proof of reinforcement. This helps explain why regret often appears years later, once social context changes and long term consequences become unavoidable.
6. Paediatric Ethics Is Not “Most Don’t Regret” Even if regret were genuinely rare, this would not resolve the safeguarding question. In paediatrics the relevant standard is whether: - the child can meaningfully consent - benefits are established with high quality evidence - risks are proportionate - less invasive alternatives exist - developmental disruption is justified Permanent losses such as fertility, sexual function, and normal pubertal development require a far higher evidentiary threshold than “most people are satisfied.”
Conclusion: “Regret is rare” functions as rhetorical reassurance, not a secure scientific conclusion. It is based on weak follow up, narrow definitions, and developmental assumptions that conflict with established child psychology. In paediatrics, the absence of recorded regret is not evidence of benefit. It is often evidence that we have not followed children long enough to see the full cost.
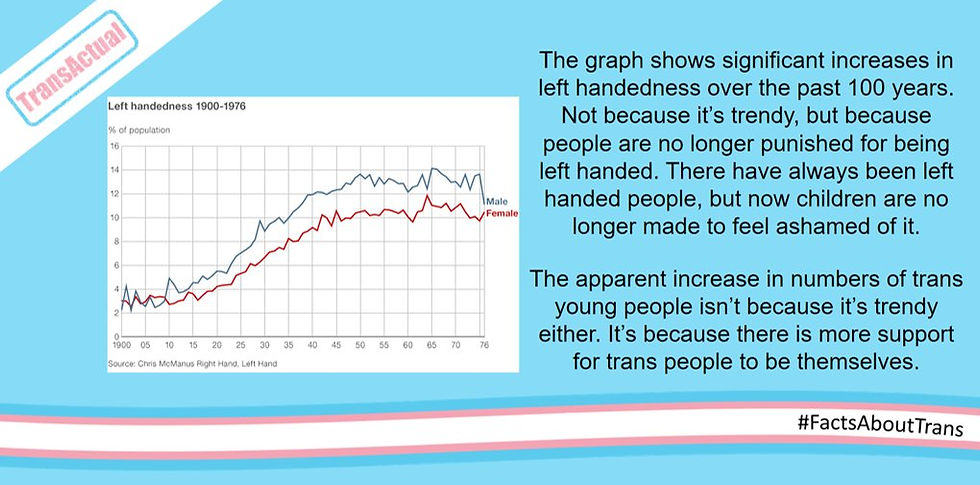
Rebuttal 10: “Trans identification is like left-handedness”
The left-handedness analogy is used to suggest that transgender identification in children is a naturally occurring trait that was historically suppressed, and is now simply being allowed. The implication is: as stigma decreases, the true underlying rate becomes visible. This comparison fails for several reasons.
1. Left-handedness is a stable behavioural trait, not an abstract identity claim Left-handedness is directly observable, behaviourally consistent, and does not require children to grasp complex metaphysical concepts. A child does not need abstract reasoning, introspection, or social narratives to prefer one hand. By contrast, “gender identity” is an abstract self concept. It requires children to interpret feelings about the body, stereotypes, and social belonging through a culturally supplied framework. Developmental psychology (Piaget, Kohlberg) shows that children’s ability to reason about permanence, category stability, and counterfactual identity is limited and gradually acquired.
2. The left-handedness curve reflects reduced punishment, not increased recruitment When left-handedness rose in the 20th century, it rose primarily because schools stopped forcing children to switch hands. That is the opposite of what is happening with gender identity, where schools and institutions increasingly introduce identity concepts, teach them explicitly, and build policies around them.
3. Left-handedness does not show identity contagion dynamics Left-handedness does not cluster by peer group, school cohort, online community, or cultural fashion. It does not spike sharply in specific demographics. It does not disproportionately affect adolescent girls. It is not associated with rapid onset patterns. Trans identification in adolescence has shown exactly those features in multiple countries: sharp increases, demographic shifts, and clustering patterns consistent with social mediation and reinforcement (Bandura, Vygotsky).
4. Left-handedness has no medical pathway attached. Recognising left-handedness does not lead to irreversible medical interventions. It carries no fertility implications, no sexual development implications, and no lifelong medical dependency. By contrast, paediatric gender pathways can lead to puberty suppression, cross sex hormones, and surgery.
5. Left-handedness does not resolve naturally Left-handed children do not “desist.” The trait is stable across development. Childhood gender dysphoria, historically, often did resolve. Longitudinal studies before widespread affirmation found high rates of natural desistance by adulthood. This alone makes the analogy inappropriate: it compares a stable trait with a developmentally fluid distress presentation.
Conclusion The left-handedness analogy works as a slogan, not as an argument. Left-handedness is a stable behavioural preference with no developmental ambiguity and no medical consequences. Paediatric trans identification is a complex, socially mediated self concept emerging in a time sensitive developmental window, often alongside comorbid distress, and linked to interventions with significant long-term implications. In safeguarding terms, these are categorically different phenomena, and pretending otherwise is a way of smuggling certainty into a domain defined by uncertainty.

Rebuttal 11: “You’re overreacting. Trans children are only a tiny proportion of children”
Even if only a small number of children socially transition, the impact is not confined to those children. In a school setting in particular, social transition functions as a public developmental script that all children are required to learn, interpret, and accommodate. Child development theory explains why this matters.
1. Schools don’t just “support” a child — they teach a framework to everyone Vygotsky and Bandura show that children learn identity concepts through social mediation, modelling, and reinforcement. In a school environment, a socially transitioned child is not simply an individual case. It becomes a lesson about what sex is, what identity is, and how to interpret discomfort. Children treat adults and institutions as epistemic authorities. If the school treats “gender identity” as a fact, children absorb it as a fact.
2. Young children think concretely, not abstractly Piaget’s work shows that primary aged children are still largely concrete thinkers. They struggle with abstract distinctions such as “sex is biological but gender is internal.” When schools introduce identity claims that contradict bodily reality, children do not process this as a nuanced philosophical position. They process it as: - confusion - contradiction - a new rule they must obey to avoid punishment This does not create understanding. It creates compliance.
3. It disrupts Kohlberg’s sex constancy development Kohlberg’s sex constancy model describes how children gradually learn that sex is stable across time. This is a normal cognitive milestone. School policies that require children to treat sex categories as negotiable, or to treat pronouns as overriding biology, interfere with that developmental process. This affects not only the transitioned child, but the entire peer group’s developing understanding of sexed embodiment.
4. Social transition is not a neutral accommodation The Cass Review notes that social transition should be viewed as an active intervention, not a harmless change. In children, identity development is time sensitive and path dependent. Once a child is socially transitioned in front of peers, the psychological and social cost of reversal rises sharply. This creates a ratchet effect: persistence increases, not necessarily because the identity is innate, but because reversal becomes humiliating, destabilising, and socially costly.
5. Adolescents are vulnerable to imitation and social reward Erikson and Marcia locate identity formation in adolescence, when belonging, status, and peer approval are paramount. In this stage, identity categories can spread socially because they offer: - a ready-made explanation for distress - a protected status - a peer community - a narrative of meaning This is not a moral claim. It is a developmental one.
6. It forces all children into “doublethink” about sex Children are not just witnessing a transition. They are being required to participate in a new paradigm: that sex can be overridden by declaration. For many children, this produces: - anxiety about saying the wrong thing - fear of punishment - the lesson that reality is negotiable if authority insists That is not inclusion. It is training in contradiction.
7. It reframes boundaries as prejudice Safeguarding depends on children learning: - bodily privacy - sex-based boundaries - that discomfort matters If children are told they must accept opposite sex peers into intimate spaces, they learn that their instincts are morally suspect and that boundaries are “unkind.” This is a safeguarding issue, not an ideological one.
8. It pressures children into speech they don’t understand Compelling children to use language that contradicts what they can see teaches: - words matter more than reality - honesty is punishable - social harmony requires self-censorship That is not healthy moral development. It is institutionalised coercion.
9. It reshapes peer dynamics, especially for girls In practice, these policies often shift the burden of adaptation onto other children, particularly girls. Girls learn that discomfort must be suppressed for social peace, while boys learn that sex boundaries can be bypassed through identity claims. Again: this is not neutral.
Conclusion: The “tiny proportion” argument misunderstands childhood development. Schools are not simply accommodating a few children. They are teaching a highly contested theory of sex and identity as fact to all children at the exact developmental stage when concepts of embodiment, category permanence, boundaries, and truth telling are being formed. In that context, small numbers are anything but trivial.

Rebuttal 12: "Children have 'Bodily Autonomy' so should be supported in transition"
The "bodily autonomy" argument for allowing "transchildren" to access medical transition (puberty blockers, cross-sex hormones, or surgeries) often frames denial of such care as a violation of fundamental rights, akin to forcing someone to live in a body that causes profound distress. Proponents emphasise compassion, self knowledge ("they know who they are"), and harm reduction, positioning gender affirming interventions as essential for well being. While this argument may carry some weight in adult contexts, its application to children and adolescents demands rigorous developmental and ethical scrutiny.
1. Bodily Autonomy Is Not Absolute in children Legal and medical frameworks worldwide recognise that children's autonomy develops gradually. Full bodily sovereignty in law is withheld precisely because children lack the mature capacity for decisions with lifelong, irreversible consequences. Because of this, society imposes strict limits on: - Elective cosmetic procedures (e.g., rhinoplasty or breast augmentation for non medical reasons). - Permanent sterilisation without compelling medical need. - Tattooing or body modification under age thresholds (often 18). - Consent to sexual activity. - Experimental or high-risk interventions without proven benefit.
These restrictions stem from developmental psychology and pediatric ethics, not arbitrary paternalism. Executive functions (impulse control, risk assessment, future projection) mature into the mid-20s, as shown in longitudinal neuroimaging studies. Adolescents prioritise immediate relief from distress over distant harms like infertility, sexual dysfunction, or bone density loss. Invoking absolute autonomy for gender related interventions ignores this established principle, treating minors as equivalent to competent adults - ie mini adults.
2. Irreversibility and the Threshold for Consent Puberty blockers (GnRH analogues) are often described as "fully reversible," but evidence shows otherwise in gender care contexts: most users progress to cross-sex hormones (90%+ in many clinic cohorts), rendering effects for practical purposes as non reversible. Even short term use disrupts timed pubertal processes critical for brain maturation, bone accrual, and psychosocial milestones.
Cross-sex hormones and surgeries introduce permanent changes: sterility, altered sexual function, and surgical risks. Developmental science questions whether adolescents can meaningfully consent to such outcomes (Piaget). Erikson's identity vs. role confusion stage highlights adolescence as exploratory and unstable, provisional identities are normative. Medicalising one provisional narrative risks foreclosing others (Marcia), especially when identity fluidity is high in untreated or psychologically supported cohorts.
3. Identity Formation Remains Fluid Adolescence involves intense, often transient commitments (ideological, sexual, subcultural). Provisional exploration is healthy; foreclosing options via irreversible bodily change during peak plasticity contravenes developmental norms. If a "stable self" is prerequisite for autonomous bodily decisions, adolescence, defined by its absence, cannot ethically authorize permanent alterations. High desistance rates in pre-pubertal gender dysphoria (historically 60–90% without intervention) and emerging data on adolescent-onset cases underscore this volatility.
4. Distress, Comorbidity, and Voluntariness Clinical cohorts show elevated rates of autism (20-30%), anxiety/depression (60-80%), trauma, eating disorders, and social isolation. Acute distress impairs decision making bandwidth; social factors (peer influence, online communities, fear of exclusion) add subtle coercion. True autonomy requires freedom from undue pressure, yet adolescents' heightened sensitivity to belonging and digital reinforcement complicates this.
5. Best Interests vs. Autonomy First Framing Pediatric ethics prioritise the child's best interests, including preserving future options, minimising irreversible harm, and supporting developmental flexibility. Autonomy is important but subordinate when maturity is incomplete. Reframing safeguarding as "denial of rights" or "harm" inverts this hierarchy.
Protecting plasticity during identity formation is protective, not oppressive, analogous to delaying elective sterilisation or high-risk experiments until adulthood. Recent policy reflects this caution: - Systematic reviews (Cass 2024, subsequent international analyses) rate evidence for benefits as low-quality, while documenting risks. - Multiple jurisdictions (UK, Sweden, Finland, Norway) restrict or pause youth medical transition outside research.
The UK's Pathways trial (intended to study blockers) was paused in February 2026 by the MHRA over safety concerns, including unquantified long term harms, calls to raise the minimum age to 14, and enhanced monitoring/consent, illustrating even research faces heightened ethical scrutiny.
6. Rhetorical Slippage Equating refusal of medical transition with "denial of autonomy = harm" overlooks that children's autonomy is already limited across domains for the same developmental reasons. The question is calibrated: how much sovereignty is appropriate for decisions reshaping reproduction, sexuality, and embodiment during immaturity? Conclusion Bodily autonomy is a powerful adult principle, but children's version is graduated, contextual, and bounded by protection from irreversible harm. Adolescence is for navigating identity crises (Erikson) through exploration and support, not ratifying present distress as sovereign via permanent medical alteration. A developmentally informed approach affirms the child's distress, provides holistic care (addressing comorbidities first), and preserves future choice capacity. This upholds genuine autonomy: the right to grow into a mature self; capable of irrevocable decisions, rather than locking in provisional ones under pressure. This stance aligns with child protection ethics and evolving evidence, not ideology.

Comments